Forum Replies Created
-
AuthorPosts
-

JR19759KeymasterHave you been affected by Superhuman misconduct? Or been the victim of a crime that the police are unable to solve? Then call Outsider Investigations. Our crack team is equiped to tackle any type of superhuman criminal case and we work seperately from the Police and Government agencies, so you can guarantee we will take your case, no strings attatched and no red tape.

Attachments:
You must be logged in to view attached files.
JR19759KeymasterNot much is known about the mysterious vigilante known as Swan-Song. He is very rarely seen and would have been considered an urban legend amongst criminals if he hadn’t also been sighted by a number of police officers and even caught on camera. But other than the fact that he exists and that he opperates in and around Emerson City, he is a mystery. One thing that is sure though, is the effect he has had on crime in Emerson. The city was, until Swan-Song’s appearance, a haven for organized crime and corruption, now many of the city’s gangs are behind bars and many of the city’s most dangerous criminals are housed in the asylum at Emerson Lake, a remote mountain lake around 15 miles out from the city limits.

Attachments:
You must be logged in to view attached files.
JR19759KeymasterThat’s awesome.
I’d love to see you try a classic “riding off into the sunset” in a simular style.
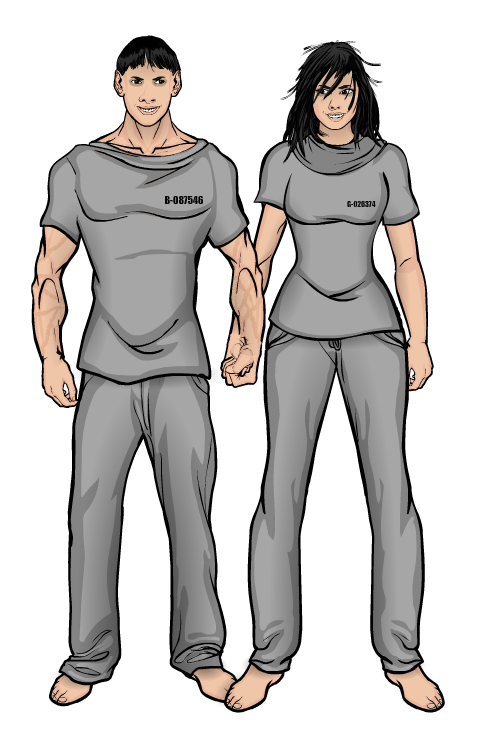
JR19759KeymasterInmate Numbers: B-087546 (m)/ G-026374 (f)
Surname: Shaw
Forenames: Paul (m)/ Julie (f)
Initial Date Of Commitment: 11/23/16
Patient Ages: 28 (m)/ 27 (f)Patient Information: Probably the most unique inmates confined within Emerson Lake, the Shaw siblings are codependant, incestuous, sexual sadists. Both are extremely dependant on the other to function on a day-to-day level, so much so that during when they were put into seperate wards upon their arrival both went into near catatonic states, refusing to talk to eat, barely acknowledging any attempts to talk to them, constantly muttering to themselves (though what they would say appeared to be directed towards their sibling). This led to a new arrangement, where they were placed in adjacent cells with a transparent perspex partition wall, so they could see each other at all times. However, this approach has not aided in their treatment and any attempts to slowly decrease their codependancy has been met with hostile resistance, leading to a catch-22 situation. Of the two, Julie is the more adjusted, able to converse quite easily with asylum staff. Paul, however, appears to have some form of learning disabilty, though any attempts to test him to discover what problems he might have and how badly he is affected are quickly derailed. He is virtually uncontrollable without his sister and is often too distracted to concentrate with her around. He is also covered with scars and marks consistant with abuse, though some of this may have been sexual in nature. Julie has admitted in interview to having sex with her brother and engaging him in fetishistic roleplay, the later of which could definately explain a number of his scars. The siblings eventually took their roleplaying to anyother level, abducting 6 men and 11 women over a 3 year period, torturing and murdering them for sexual pleasure. These acts would eventually lead to their being commited to Emerson Lake, though their arrest is somewhat of a mystery. Accounts of Police officers who worked the case say that a large amount of the evidence in the case was sent to them annonymously and the siblings were not captured by any officer working in their district, instead they were found tied up outside the Police Department one morning with photos of them commiting their crimes. Neither would speak after the incident, instead muttering to each other about “the man that hurt (them)”.
Patient Speech Recording:
(Recording made by Doctor Robert Levering 1 hour before the break out at Emerson Lake Asylum. Doctor Levering was killed by inmates during the breakout. It is unknown as to whom “the man” the Shaw siblings are refering to in their conversation is, but Doctor Levering would note that he did not believe they were refering to anyone in the Asylum when he informed security of the incident. It is possible that “the man” they refer to is the same man they refered to when they were arrested, but we cannot know for sure and the chances of an outsider gaining access to Emerson Lake without permission is practically impossible. No further security transmissions were made from Emerson Lake after this).
Sister
Brother
The man is coming.
Yes, he is coming.
He hurt us
But we won’t let him hurt us again
We will hurt him
Yes, we will hurt him
We will hurt lots of people
Yes, my love we will.
Doctors and nurses and guards and policemen!
Yes, patience darling, we have to wait a little while longer.
But I don’t want to wait.
Just one more night and we’ll be free, free to hurt, free to kill and free to love. Can you wait just one more night for me my love?
Attachments:
You must be logged in to view attached files.August 14, 2017 at 1:59 pm in reply to: Lull-carae's works – Place where criticism is welcome #147194
JR19759KeymasterAwesome
JR19759KeymasterInmate Number: E-128760
Surname: Richards
Forename: Henry
Initial Date Of Commitment: 05/02/15
Patient Age: 38
Gender: MalePatient Information: Richards is an interesting case. He suffers from Narcissistic Personality Disorder, which has exegerated his sense of self-worth and his need for admiration alongside a trait that sees him project his own views onto other people, leaving him almost unable to see or hear critisim. This part of his psychological profile is complemented by an extraordinary delusion, which sees him take on the role of a King figure based upon the King of Hearts character from your standard playing card deck. These conditions would not be so bad on their own but become concern when two other aspects of Richards personality is taken into account. He is ruthlessly intelligent and exceptionally charismatic, which allows him to easily manipulate people. He managed to gather himself together a small criminal gang (which he based off of playing cards, as per his delusion, assigning each member of his gang a rank and position based off of a corresponding card) and transform it into a nation-wide operation of thieves, money launderers and drug dealers, with himself at the top. The other aspect of his personality that makes him so dangerous is his unpredicable temperament. For all his charm and intelligence, Richards is capable of horrific acts of brutality (as seen in the Vasquez case of 2012-13) if he feels provoked. He was commited to Emerson Lake after his gang was sold out by the brother of a former member that Richards had killed. Richards lawyers argued insanity as a way of ensuring Richards didn’t see death and it is hard to argue that the man is, by definition, insane. However, it should be noted that at no time should staff underestimate him. His sanity may be questionable, but his cunning is not and he is for more mentally able than most inmates in our care.
Patient Interview Exerpt:
Doctor: Taped Patient Interview with Patient E-128760: Richards, Henry. Session 1. Conducting the interview is Doctor Clifton Love. Hello Henry, how are you today?
Richards: Good afternoon Doctor. Unfortunately, I cannot say that today has been a particularly good day, but manners compell me to wish you such.
Doctor: How has today not been good Henry?
Richards: Well, one cannot pretend that ones accomodation is anything but unsatisfactory. You have me locked up in this place with common criminals and lunatics, it just won’t do. I am used to a certain level of luxury and that requirement is not being fulfilled. Now, I am aware that an establishment such as yourselves cannot afford to serve lobster or kobe beef, so one does not expect it. However, the quality of the matresses is disgraceful and the pillows offer no neck support. And the lack of privacy is insulting. The fact that I have to spend my time in a room that has a window in the door so as anyone passing by can see me at all times is not acceptable. And do not get me started on the lack of respect shown around here. I should be address as either Mr. Richards or Your Majesty at all times, as befitting of my royal stature. The fact that someone of your level of intellect and professional standing is refering to me by my Christian name is unprofessional and childish, you should be ashamed of your self.
Doctor: That’s how things work around here Henry. You are here to be treated for your delusions…
Richards: (makes disapproving and disbelieving noise)
Doctor: And as such you are to be treated just like any other patient. You have exactly the same sort of cell as everyone else, the same sort of pillow and mattress. The window in the door is so the guards can see if you are having a seizure or trying to hurt yourself, which does happen with a number of our patients. And we call you by your first name because that is protocol. It helps settle some of the more disturbed patients. Unfortunately, we have to follow protocol. I’m sure you, of all people, would understand that, surely?
Richards: Yes, quite. We all must adhear to protocol. I insisted on it with my pack. But you must understand my plight here doctor. I get awful cramps if I do not sleep properly and I struggle so with these condtions. My body just isn’t adapted to this sort of lifestyle.
Doctor: (sighs) I will talk to the Infirmary, see if we can get one of the MD’s to come down and examine you. If they see there is something wrong, we might be able to put in a request for special bedding. However, this would be conditional on good behaviour.
Richards: Of course. Even I would not expect something for nothing.Attachments:
You must be logged in to view attached files.
JR19759Keymaster@Herr D- Well, considering that none of the inmates here have tenticles, I’m pretty sure it is a fair assumption that there are no comparisons 😉 Cheers
Inmate Number: C-019867
Surname: Peterson
Forename: Abel
Initial Date Of Commitment: 08/11/14
Patient Age: 32
Gender: MalePatient Information: A High Functioning Psychopath and Sadist who was commited to the asylum after a spate of homocides where he would mutilate his victims sexual organs and remove their eyes before killing them, leaving his signature X cuts across both eye sockets. Peterson would find his victims, usually young socially active women, at clubs, where he would charms them into going home with him. In interviews, he has shown no remorse for his crimes and even less regard for his victims or their families, admiting that he only killed for fun and the more horrific aspects of his crimes where just for attention. Despite his obvious mental deficiencies, Peterson is smart. The scars across his face came from an incident of self-mutilation early on in his incarceration at the asylum, but were made so that they were not deep enough or serious enough to cause him any visual impairment, but just deep enough for him to be taken to the infirmary. When in the infirmary, he overpowered the doctor and his guards and attempted to escape through the staff area, though his attempt failed.
Patient Interview Exerpt:
I crept up like a disease, looking for a girl who was trying to be seen. And her heart was trying to bleed and she was taking the right road just by talking to me. Hell, she thought she could tear my skin from bone, just cause it was cold and she needed a coat. “Don’t tease me”, just start digging the hole, start digging. Oh, she was getting so sleepy that night and she wanted to go home but she didn’t have a ride. There was no time to waste, I couldn’t touch for free, my salt her sweet.
And we were there, and I was every question that never had an answer. I saw right through her. She never even noticed that there always was a reason that we were never meant to be left alone.Attachments:
You must be logged in to view attached files.
JR19759Keymaster@ Blue Blazer- Thanks, I try.
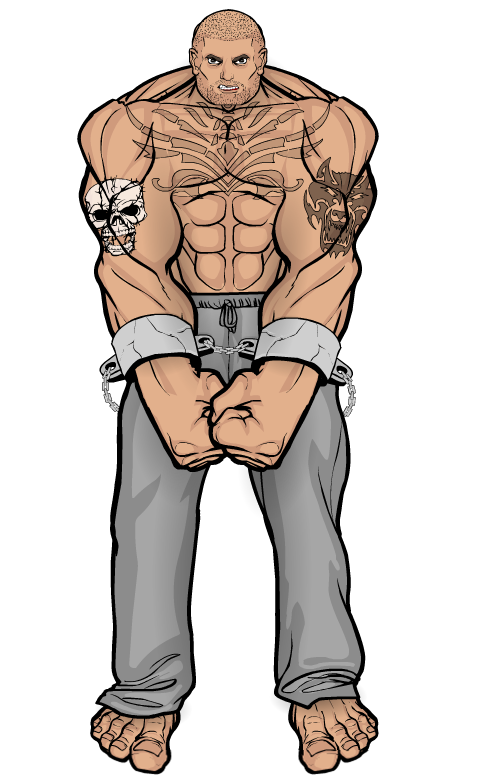
Inmate Number: D-134256
Surname: Murr
Forename: Arnold
Initial Date Of Commitment: 05/05/12
Patient Age: 36
Gender: MalePatient Information: One of the asylums most difficult inmates, due to his size, strength and temprement, Murr was commited to Emerson Lake after a psychiatry expert classified him as mentally unstable and a low functioning sociopath with intermittent explosive disorder (a mental condition that causes a person to suffer explosive outbursts of anger often disproportionate to the situation they are in). He was originally arrested when he for killing a man during an arguement. The victim was later described by the coroner as having “injuries consistant with the victim of a vehicular assault”, so brutal was Murr’s attack. His treatment thus far has been unsuccessful. He does not respond to behavioural therapy and often requires forceful encouragement to take his medication (anti-depressants, mood stabilizers and seratonin inhibitors alongside Lithium and Carbamazepine). He requires almost constant physical and chemical restraint and has been put into solitary confinement on numerous occassions for attacks on staff and other inmates (including the incident on 08/12/14 where he put a guard through a partition wall between two cell blocks).
Patient Interview Exerpt:
Doctor: Taped Patient Interview with Patient D-134256: Murr, Arnold. Session 3. Conducting the interview is Doctor George Collado. Hello Arnold, how are you doing today?
Murr: (silence)
Doctor: How are you doing today?
Murr: (silence)
Doctor: Look Arnold, you’re in a safe place. We want to help you in any way we can, but you need to talk to us, we can’t help you otherwise.
Murr: You wanna help?
*(crashing noise of wood being splintered followed by indeterminant shouting and sounds of multiple people fighting)*

Attachments:
You must be logged in to view attached files.
JR19759KeymasterDude, that’s pretty damn awesome.
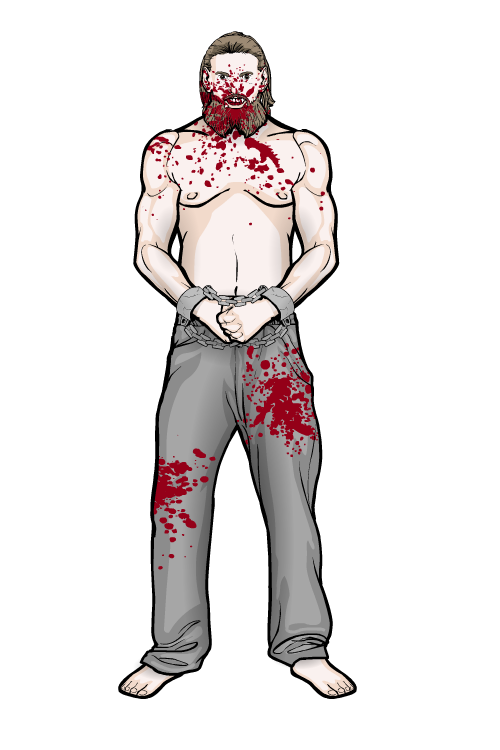
JR19759KeymasterInmate Number: C-765947
Surname: Gullan
Forename: Victor
Initial Date Of Commitment: 03/08/12
Patient Age: 47
Gender: MalePatient Information: A cannibal, Victor Gullan was commited to the Emerson Lake Asylum upon his arrest for a string of homocides over a two decade long period. Much of what was left of his victims was found in various places around the house in which Gullan lived, though a large amount of each of the desceased was missing due to both decay and Gullans own eating habits. Based on information gained from interviewing Gullan, it can be concluded that this behaviour stems from his childhood as well as brain damage from a childhood incident. His family lived below the poverty line and often struggled to afford enough food to feed themselves. Gullan also says that his elder brothers physically abused him as a child and would steal any food he had, leaving him to scavenge for anything edible he could find. He claims to have eaten rats, cats, dogs and pigeons to survive before stumbling onto a dead vagrant at one point during his early teens. Gullan is not clear on why he decided to eat a dead human, but it is clear from medical examinations conducted upon his arrival at the asylum that around this time Gullan recieved a fracture to his skull from a heavy blow to the head which caused a traumatic brain injury (TBI) to his left frontal lobe. This injury is likely to have caused problems with Gullans descision making process, as seen in other cases of TBI in this area. He shows other symptoms congruant with the injury, problems with his memory, social deficiencies, impulsive behaviour and slight problems with his motor functions. Whatever the cause of his cannibalism, it is abundantly clear that the habit has become all-consuming (a symptom of cannibalism long documented, often likened to drug addiction) and it has been hard to persuade Gullan to eat “normal food”. He has had to be feed intravenously on a number of occasions in the asylum infirmary to prevent him starving himself to death and, early on in his tenure, he was regularly under physical and chemical restraint due to his numerous attacks on hospital staff and other inmates, during which he would attempt to bite their arms, legs and shoulders. These attacks have become less frequent as his treatment has progressed, but there is still a worry that he may have an incident at any time, especially whilst he still refuses to eat.
Patient Interview Exerpt:
I like chops the best. Take a slab off the back, fry it up with some butter, pinch o’ salt n’ pepper, like you would a pork chop. Ribs ain’t bad, but not much meat on ’em and not as easy to butcher. You get some good meat off legs mind. That guard there, he looks like he’d have some good eatin’ from his legs. You wouldn’t though, too fat. You’d taste good an’ all, but I’d be pickin’ you out my teeth for weeks.
Attachments:
You must be logged in to view attached files.
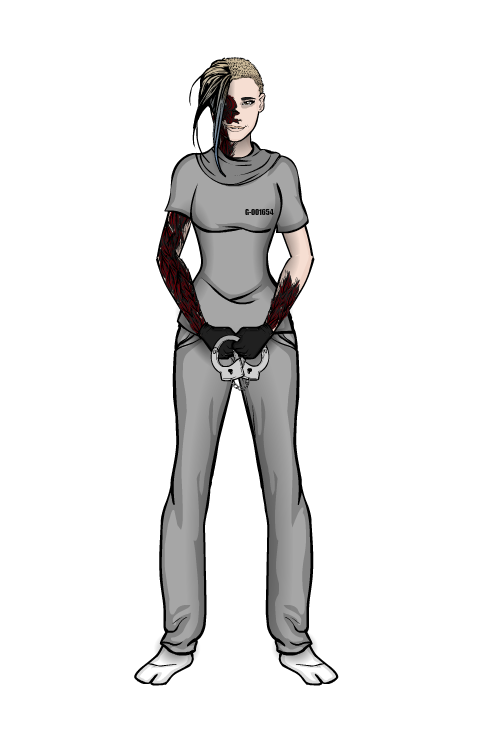
JR19759KeymasterInmate Number: G-001694
Surname: Dyer
Forename: Amy
Initial Date Of Commitment: 11/06/15
Patient Age: 26
Gender: FemalePatient Information: Dyer appears to suffer from DID (Dissociative Identity Disorder, commonly known as Multiple Personality Disorder). She certainly shows a convincing case to suggest one markedly different alter alongside the host personality. The host, Amy, is a rather meak and shy girl with a pronnounced stutter, whilst the one identified alter, Amanda, is highly volatile and aggressive, with a tendancy towards pyromania. As of yet, staff are only aware of these two personalities, and there have been no hints of any others. It is obvious from documented evidence (police reports and child services documentation) that Amy suffered a great deal of physical and mental abuse during her formative years, before she was taken away from her family at age 6. We can speculate that Amanda formed around this period, as it fits the developmental time frame for the disorder and events from this time could also explain her pyromania, as a barn fire at her family’s farm killed her elder brother and family dog during her early years. In interviews with asylum staff, Amanda has admitted to going out and starting fires in local properties as a teenager to cope with the stress of being in the foster care system. Evidently, these fire-starting trips would become more regular and more reckless as she grew older. When questioned about this, Amy claimed she has no knowledge, as is congruant with cases of DID. Dyer came into the asylum’s care after being caught in one of Amanda’s arson attacks. She was badly burnt in the incident, however, treatment at the local hospital became complicated as Amanda refused skin grafts and even attacked the doctors that treated her, whilst Amy was in a near catatonic state due to the shock of waking up in the hospital badly burnt with no idea what had happened for the entire time her personality was in control. Fortunately, since being commited, Dyer has shown great improvement, through a treatment schedule of anti-depressants, anti-anxiety drugs alongside regular cognative and creative therapy sessions and incidents of Amanda taking control have become few and far between. However, Amy has become quite scared of Amanda since becoming aware of her second personality and there is still a high risk of a mental break when she is exposed to high stress situations (see 07/07/16 incident. Amanda nearly blinding Doctor Roberts after Amy recieved the news of a former foster mother’s death) and it is also worth noting that, early on in the treatment, Amanda would regularly self-harm, which lead to the application of chemical and physical restraints to Dyer whenever she was left unsupervised.
Patient Interview Exerpt:
Doctor: Taped Patient Interview with Patient G-001694: Dyer, Amy. Session 9. Conducting the interview is Doctor Jeremy Hollingshead. Hello Amy, how are you today?
Amy: H-hello Doctor. I-I’m… okay I guess…
Doctor: Doctor Levering tells me that you’ve been very well behaved since our last session. Taking your medication, staying out of trouble, you haven’t had an incident in a few months now, is that right?
Amy: Y-yes d-doctor.
Doctor: Yes, you have made very good progress. Hopefully we will soon be at the stage where we can get those burns of yours taken care of.
Amy: *whimpers*
Doctor: What’s wrong Amy? Do you not want the Doctor to treat your burns? I thought you said that they were still painful? If we get them seen too we can decress your medication and start the next stage of your treatment. Do you not want that?
Amy: I-it’s not that s-sir, i-it’s just… s-she d-doesn’t like t-the i-infirmary. A-and I d-don’t w-want her t-to g-get out again y-you see. I’m a-afraid t-that s-she’ll hurt s-someone again, or hurt m-me…Attachments:
You must be logged in to view attached files.
JR19759KeymasterInmate Number: A-103875
Surname: Doe
Forename: John
Initial Date Of Commitment: 06/05/13
Patient Age: (unknown)
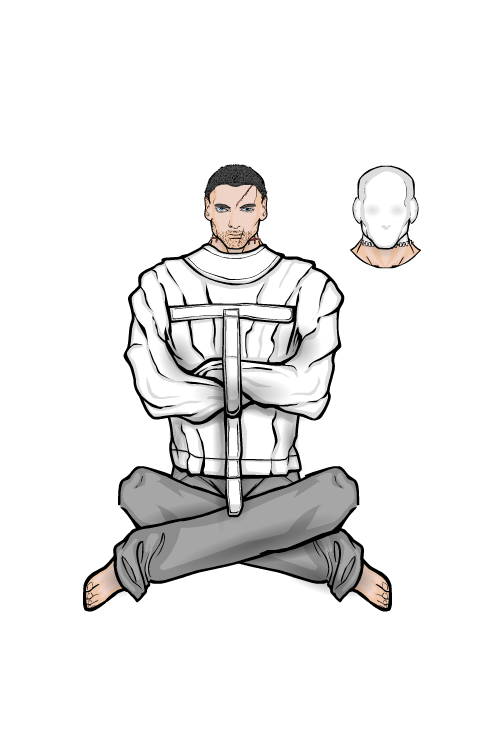
Gender: MalePatient Information: Inmate A-103875 is a frustrating case. There are no records of him in any database, no birth registration, no social security, no known place of residence, any information from before his incarceration. Questioning him about his lack of background has proven fruitless for both police and medical professionals. He displays many traits typical of paranoid schizoprenia, intense feelings of persecution manifested around modern democratic society (which the inmate proclaims is corrupted and conspires against those without power) and claims to hear voices telling him that he is being watched and being hunted. He also claims that the voices tell him that it is his purpose in life to bring down the current system and replace it with an anarchic system without government, where everyone is equal. Interestingly, the one piece of information the inmate has given away about his past is that he claims that his parents were taken away by the government when he was a child, though whether this is ture or just another persecutorial delusion is unclear as the inmate seems purposefully vague about the details. His commitment to the asylum came after the inmate commited a spree of terrorist attacks against a number of public and private buildings in the greater metropolitan area, including the City Hall and the First National Bank. At the time of his arrest, he was wearing a plain white gauze mask over his head, which was sewn to his neck to keep it in place. When asked about the mask, his only reply was that it was a gift and refuses to say who helped him sew it on (as it was obvious that the inmate did not sew it on himself). Unfortunately, little knowledge can be gained from interveiw sessions with the inmate as he is highly tempremental. If he is in a good mood, he will talk a little, but only about his persecution delusions. If he is in a bad mood, he is highly likely to lash out, meaning he has been issued with physical restraints for any interactions with staff. It is also worth noting the effect the inmate seems to have on other patients. Many of the more disturbed patients appear to gravitate towards him and he has a marked effect on how effective their treatments can become, with any sustained contact leading to an marked increase in patient agression. For this reason, the inmate has been moved to a secure solitary confinement away from other high risk patients.
Patient Interview Exerpt:
Society’s a sickness.
And I am the cure.Attachments:
You must be logged in to view attached files.
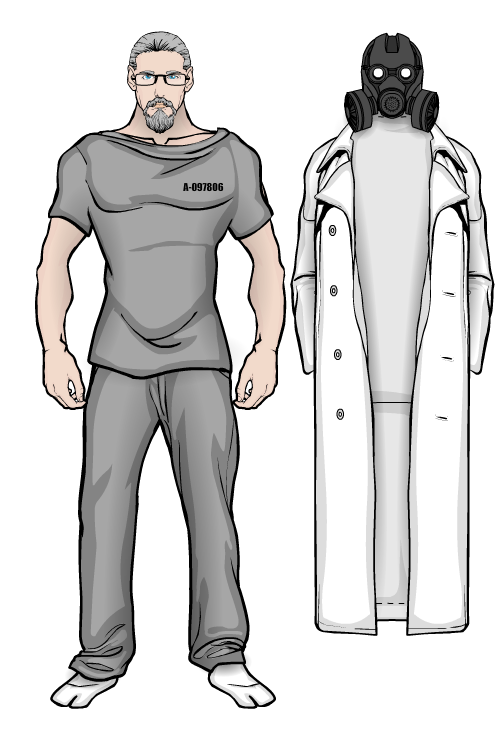
JR19759KeymasterInmate Number: A-097806
Surname: Chambers
Forename: Leonard
Initial Date Of Commitment: 01/12/11
Patient Age: 58
Gender: MalePatient Information: A former practicing psychologist and psychiatrist, Chambers was commited after it was discovered that for years he had been conducting numerous illegal and unethical psychological studies on unconcenting human subjects. The charges brought against him include multiple counts of kidnapping, false imprisonment and torture as well as a number of charges of incitement to commit homocide. His “studies” concerned human adaptation to extreme mental stimuli, in effect his aim was to see how quickly he could drive his subjects insane through a mixture of physical and mental torture assisted by large doses of psychadelic drugs administered through injestion, injection and evaporated into the air within Chambers compound. Chambers lack of remorse or empathy for his victims suggests a degree of the psychopathic, which was apparently enough to convince the forensic expert and jury to agree with his plea of insanity. His case is one few specialists here at the Asylum particularly enjoy dealing with, as his knowledge of the profession and unnerving presence has an effect on even the most experianced member of staff.
Patient Interview Exerpt:
Sanity is a precarious balence, you see. There is potential for it in everyone, but the limit is different for everyone. For someone it could be just one bad day sending them over the edge, for someone else it could be a build up of madness over time. That’s what interests me, what it takes for even the most sane person to succumb. That’s why I ran my experiments. Of course, you wouldn’t understand, how could you. Medical science and the field of psychology are far too rigid to understand my work, far too wrapped up in ethics and ensuring patient safety to make any meaningful discoveries. How can you truly discover the dark secrets of the mind if you are bound by ethical standards? As any good chef will tell you “you can’t make an omlette without breaking a few eggs”. But of course, being in here is no hinderance to me. So many test subjects, controlable variables of excellent quality and quantity, both sane and insane. Now tell me, Doctor, how long can you last?
Attachments:
You must be logged in to view attached files.
JR19759KeymasterEmerson Lake Asylum, Palmer County
Situated on an island in the middle of Emerson Lake amongst the mountains and forests of Palmer County, Emerson Lake Asylum was a state of the art correctional institute equipped to house some of the world’s most dangerous inmates from prison systems across the country, all of whom are criminally insane. But then something went wrong. The inmates got out and now the lunatics are running the Asylum. Fortunately, the Asylum’s state of the art security system ensured the facility went into lockdown, containing the inmates, but that has led to a new problem. The few staff that survived the initial breakout now have very little chance of escape and the police are locked out by the very same system that’s keeping the inmates in.
Please find below information on inmates of special interest. Engage with caution.
Inmate Number: A-117629
Surname: Brady
Forename: Bryant
Initial Date Of Commitment: 07/05/14
Patient Age: 43
Gender: MalePatient Information: Brady was commited to Emerson Lake Asylum by court order after his council pled insanity against a charge of 18 homocides between the years 1992 and 2013. His crimes consisted of the rape and decapitation of men and women between the ages of 15- 25, with his victims usually being blonde haired (or dyed blonde) and of slim figure. He would collect the heads of his victims and preserve them as trophies, throwing out the bodies in secluded public areas such as woodlands or back alleyways. His method of killing would gain him the nickname “The Headhunter” from the press. There is documented evidence of abuse during his childhood by both his father (a small town preacher) and by some elder students at his high school, both of which Brady corroberates. His father went missing in 1987 and, whilst Brady admits to the crime now, there was no evidence at the time of foul play on Brady’s part and a body was never discovered. This, combined with local knowledge that the man was a drunkard and a bully with many enemies, led to the case going cold.
Patient Interview Exerpt:
They say God loves us all, each and every one of us. But that’s not true. God does not love me. He never did. My Father was a man of God. He used the Lords words to violate me, to break me, to make me his own. He would go out and preach words of love and tolerance, but could only show his son how to fear and hate. But he taught me a very important lesson, that God does not care. And if God does not care then what do you have to fear in hell? So I killed him. I killed my father and I killed God. And in that moment I became God. I brought judgement upon all those filthy queers and whores who spent their days looking down on me, laughing at me, making me feel worthless. If your God will not judge the sinful then the new God will.Attachments:
You must be logged in to view attached files.
JR19759Keymaster@Streetwise- Are you masking the dress to the circle or the circle to the dress? It sounds like you’re doing the later. The way masking works is that the item you currently have selected is the item that will be masked onto the item you click with the masking tool. If you have an insignia selected and you click on a top with the masking tool you’re going to mask that insignia to that top (it’s how you get patterns on clothing items). However, if you do it the other way round (have the top selected and click on the insignia with the masking tool) the top should only show within that insignia, as in keric’s demonstration. That’s the only thing I can think of that might be going wrong. The top might be disappearing because you have the insignia layered above the top, in which case just move the insignia to the back most layer (or set the alpha to 0% in the colour tab on all three colours), or the insignia is positioned in a place that the top isn’t (e.g. the top is in its default position and the insignia is off past the left arm or something like that). I haven’t heard of any masking bugs that cause items to disappear when masked so those are the only things I know of that would be causing that problem.
Hope this helps.
-
AuthorPosts